MUST-READ Selection(s):
FACTS Are NEVER 'Harassment'
On Incentives And Ridiculous Tropes


The content on this site is provided without any warranty, express or implied. All opinions expressed on this site are those of the author and may contain errors or omissions. For investment, legal or other professional advice specific to your situation contact a licensed professional in your jurisdiction.
NO MATERIAL HERE CONSTITUTES "INVESTMENT ADVICE" NOR IS IT A RECOMMENDATION TO BUY OR SELL ANY FINANCIAL INSTRUMENT, INCLUDING BUT NOT LIMITED TO STOCKS, OPTIONS, BONDS OR FUTURES.
Actions you undertake as a consequence of any analysis, opinion or advertisement on this site are your sole responsibility; author(s) may have positions in any firm or security discussed here, and have no duty to disclose same.
The Market Ticker content may be sent unmodified to lawmakers via print or electronic means or excerpted online for non-commercial purposes provided full attribution is given and the original article source is linked to. Please contact Karl Denninger for reprint permission in other media, to republish full articles, or for any commercial use (which includes any site where advertising is displayed.)
Submissions or tips on matters of economic or political interest may be sent "over the transom" to The Editor at any time. To be considered for publication your submission must be complete (NOT a "pitch"), include full and correct contact information and be related to an economic or political matter of the day. Pitch emails missing the above will be silently deleted. All submissions become the property of The Market Ticker.
Considering sending spam? Read this first.
There is excuse-making and then there is an entire damned industry that works its level best to asset-strip you to your underwear so your fat ass (and the rest) hangs out.
“The key point is that you can be on TV, you can lose enormous amounts of weight, you can go on for six years, but you can’t get away from a basic biological reality,” said Dr. Schwartz, who was not involved in the study. “As long as you are below your initial weight, your body is going to try to get you back.”
Well sure, if your "path" to weight loss is to eat damn near nothing (e.g. starve) and run your metabolic demand through the ceiling by engaging in extremely intense exercise.
Look at the quotes: "It's hard. The cravings are there."
But the kernel of truth is right here:
“There is a lot of basic research we still need to do,” said Dr. Margaret Jackson, who is directing a project at Pfizer. Her group is testing a drug that, in animals at least, acts like leptin, a hormone that controls hunger. With weight loss, leptin levels fall and people become hungry. The idea is to trick the brains of people who have lost weight so they do not become ravenous for lack of leptin.
Pfizer wants to sell you a drug, of course.
But what if you learned that hunger is largely regulated by leptin, leptin response is largely mediated by insulin levels, and it is what you eat, not how much, that is almost-entirely responsible for insulin levels?
Guess what: That all happens to be true.
What is being discussed here is that the contestants on the show The Biggest Loser basically poisoned their metabolism through the path they engaged in -- that is, extreme caloric restriction coupled with intense exercise.
But the "big lie" is right here:
“What was surprising was what a coordinated effect it is,” Dr. Proietto said. “The body puts multiple mechanisms in place to get you back to your weight. The only way to maintain weight loss is to be hungry all the time. We desperately need agents that will suppress hunger and that are safe with long-term use.”
Agents, of course, means drugs. Yeah that's a great idea -- hand over $10,000 a year forever to someone for a pill that will probably have side effects that destroy your life (eventually.)
Look at what they had these people eat:
His routine went like this: Wake up at 5 a.m. and run on a treadmill for 45 minutes. Have breakfast — typically one egg and two egg whites, half a grapefruit and a piece of sprouted grain toast. Run on the treadmill for another 45 minutes. Rest for 40 minutes; bike ride nine miles to a gym. Work out for two and a half hours. Shower, ride home, eat lunch — typically a grilled skinless chicken breast, a cup of broccoli and 10 spears of asparagus. Rest for an hour. Drive to the gym for another round of exercise.
Mother of God will you stop killing yourself?
Look folks, fat in the diet is not fat on the body. This sort of "diet" is nothing other than starvation and it's stupid.
What's the problem? Right here:
His slow metabolism is part of the problem, and so are his food cravings. He opens a bag of chips, thinking he will have just a few. “I’d eat five bites. Then I’d black out and eat the whole bag of chips and say, ‘What did I do?’”
Get the damned chips out the house!
Oh, and the rest of the carbs.
You're not sick because you're fat (and cut the "shaming" crap, facts just are) you're fat because you're sick and you're sick because you refuse to stop eating things that make you that way.
Look folks, I know you don't want to hear it because you're all looking for a drug and an excuse.
That's why you lose 10, 20 or 30lbs, then put it all back on with interest.
You can't stop eating pasta, potato chips, pizzas and bread.... Really? You're willing to trade being fat and ultimately developing diabetes causing you to have your toes chopped off one by one as they turn gangrenous, along with losing your eyesight and ultimately your life, rather than getting the damned potato chips out of your house and not calling Papa Johns or Dominos? REALLY?
You do understand that your body's metabolic system is capable of handling quite the level of insult before it breaks, right? That you "pass" the common glucose test (OGTT) or have a normal (or marginal) A1c today does not mean you have not accumulated decades of such damage and that while there is a test to determine this (OGTT+insulin assay) it's expensive and insurance will not pay for it since it doesn't diagnose a disease that is occurring now.
You do understand that the majority of adults in America and damn near everyone over the age of 60 are metabolically compromised by decades of eating fast carbohydrates and vegetable oils, even if you do not today show evidence of diabetes and related diseases, and that if you are overweight, even only somewhat, or obese it is a virtual certainty you're one of them irrespective of age, right?
I've been there and done this over the space of a couple of decades. I too poisoned myself because I was ignorant and believed that if I ate fewer animal fats, more vegetable oils and more carbohydrates while simply exercising more and eating less I'd lose weight and keep it off -- along with avoiding said disease.
Everyone who told you this either didn't know what the hell they were talking about or was lying. The results were the same as they are for most of you -- slowly but inexorably increasing body weight.
Then I changed what, not how much, I ate and my body's regulatory system healed over time. Is it completely healed? I'm sure it's not, and if I was to go back to eating how I used to eat all the weight I lost and probably more would come right back on -- and quite quickly too.
But guess what? You can do it too. I don't care how fat you are now or how long you've been fat. I don't care if you've yo-yo dieted before, or engaged in some sort of extreme attempt to lose weight.
You're overweight because you have poisoned the regulatory systems in your body that control your desire to eat. You almost-certainly poisoned them unintentionally but whether it was intentional or not does not matter; what matters is that it happened and unless you change what you eat the damage will continue to accrue over time and at some point it is very likely it will manifest itself as clinically-diagnosed disease.
To succeed in allowing your body to repair itself to the degree it can, however, you are going to have to do two things: Stop making excuses and stop looking for answers in a damned pill bottle -- or a surgeons office.
The answer is found in what, not how much, is in your pantry and refrigerator.
Read this article. Bookmark it, print it, whatever.
Go through your house -- pantry, fridge and freezer. Throw anything on the "don't eat list" in the trash can and never let it come back into your home or pass your lips when you are somewhere other than at home.
Go to the store once you've thrown everything away on the "don't eat list" and re-stock your fridge with things on the DO eat list. Note that almost none of them will go in the pantry because the pantry is for things that are shelf-stable and processed. A few will go on the counter that are going to get eaten within a couple of days but the rest go in either the fridge or freezer.
Don't tell me that you can't do it because you can do it. You can do it when you're home and you can do it when you're eating away from home. If you absolutely must have a sub sandwich when out go to Jimmy Johns and have them make it as a wrap; they will, in lettuce -- or if you want then go to Subway and have them make your "sub" as a salad (same thing but with the lettuce chopped up and thus less-convenient to eat "on the go.")
If you're overweight your pants will shortly try to fall off, but more-importantly your body knows how to regulate its caloric intake if you stop poisoning the mechanisms that control it. When you reach an appropriate weight - which is not one where you're "large", but rather a body mass that looks like a normal, not-fat person in every case (no, you're not "special" in that regard: You're not "big-boned", you're fat) the weight loss will stop all on its own without you making a conscious decision to do so.
Here's the thing, however: You can't get there from here if you "diet" because as soon as you stop "dieting" you will go back to poisoning your body's metabolic signalling system and the weight will come right back on. In fact it may come back on faster than ever because some of the damage you've accumulated is probably permanent.
This is not a matter of "blame" it is a matter of fact -- whether you undertook what you did because you were stupid, you got bad advice from so-called "professionals" or any other cause doesn't matter.
You are an adult and thus you are responsible for the outcomes that occur when you listen to various people no matter who they are.
If you take someone's advice and it doesn't work but you keep doing what you were told would work why in the hell would you keep listening to them?
Look folks, do it for 30 days. That's all. I'm no doctor but I can tell you what works because it did after a couple of decades of the "conventional advice" not working. I can also point you to the comments here from others who also had it work with some of them having ridiculously dramatic results when it came not so much as to weight (in that short amount of time) but metabolic markers of serious disease such as their blood sugar. This isn't something that was a "fad" or an undertaking that I "recently" did and thus can't give you any sort of honest answer on whether the weight I lost will stay off.
You want to know how many people I've run into who have actually done this and not had it work? Zero. Every one of the people I've been acquainted with that failed has admitted they just didn't do it. They ate the pasta. Or the potatoes. They called Dominos and ate the pizza. Or they just "had to have" the pie. Or sugar in their coffee. They had the craving, they had a bad day exercising and had to "add back" some carbs (even though they were less than a week into it), and on and on. Rather than tough it out for a few days, literally, knowing it would go away in a few days to a couple of weeks (like a cold does) if they just kept at it, they didn't.
It didn't fail -- they simply didn't do it and they admit it.
I changed my lifestyle in this fashion in 2011. I used no drugs, no doctors and no surgical interventions -- nothing other than what I stuffed in my pie hole and had in my house. I did it despite having a kid at home at the time who refused to give up her Doritos, M&Ms and similar.
Despite the bad stuff being present I didn't eat them, choosing instead to reach for the broccoli or piece of leftover zero-carb roast.
If you're one of the millions of Americans who have heard that it's all "hormonal", that you need "help", that you have a "damaged" metabolism and "it's not your fault" or that nothing other than invasive surgery or drugs (and perhaps not even then) will make a long-term difference what do you have to lose by trying?
Do you really think that a month or two of changing what you eat is going to do some critical damage that all those years of piling on the pounds hasn't? Are you really too lazy to go spend under $50 for instrumentation that will (largely) last virtually forever to test a hypothesis on your body and your metabolism and give you objective results by which to measure whether it works or doesn't? I don't think there's anywhere in this country that's more than a 20 minute drive from a WalMart these days and if there is Amazon covers every US address within a couple of days (even without Prime) so there's simply no excuse other than willful refusal.
You can't argue with objective numbers so if you don't have them because you won't go buy the $20 worth of stuff to obtain them in the privacy of your own home where nobody else can ever see them then the only excuse is that you are consciously refusing to put such a change in eating habits to an objective, personal test.
If you're happy with being overweight or obese, or worse you expect someone else to either fix it or give you a pill then shut your pie hole and deal with the consequences of your choice. A choice that, I remind you, given our corrupt and extortionate medical system will bankrupt you as well as having a high probability of making you both sick and ultimately dead.
Or, for nearly zero money you can change, what, not how you eat -- not as a "diet" but as a lifestyle and as a side effect it is highly like that your pants will fall off.
Your choice.
The medical industry doesn't want you to read this.
Nor does the food industry.
But you should read it, and let it sink in.
There is a lot of BeeEss flying around about low-carb eating. Here are some common myths and truths related to this lifestyle.
- Myth: It's a "fad diet." Eating low-carb is a lifestyle, not a diet and it is not a fad. In fact humans, prior to the discovery of high-density agriculture, almost-exclusively ate in this fashion. A "fad" is an unproved and new way of doing something without examination as to validity. It is in fact the modern mania with vegetable oils, nearly none of which exist in nature, along with other highly processed foods such as cereals and sugar-laden things, driven by literal billions of advertising dollars, that is the fad. Nobody spends a billion dollars advertising broccoli crowns on TeeVee!
- Myth: Low-carb eating means not eating vegetables and fruits. Nonsense. For nearly everyone who decides to eat low-carb their consumption of vegetables greatly increases, especially when it comes to green vegetables. There is no restriction whatsoever in the consumption of things such as spinach, broccoli, brussels sprouts, cucumbers and its soaked-in-vinegar friend the dill pickle, various forms of peppers and similar. Small, nutrient-dense fruits and berries, along with nuts, are also compatible in amounts comparable to that which would be found "in season" naturally.
- Myth: Low-carb eating means not getting enough fiber. Oh really? All those vegetables are an insufficient source of fiber? Like hell; what's missing is the artificially-added back fiber that people love to crow about in things like bread, which wasn't there in the first place due to all the processing. I suppose if you want to eat what amounts to cardboard (cellulose) that has been put back into a processed food so it can claim to be "high fiber" then yes, it means "not getting enough" but the last time I checked cardboard wasn't a naturally-occurring thing nor would you find it tasty -- unless it was slathered with sugar. Guess what gets added to these "foods" to make all that added-back fiber palatable? Yep.
- Myth: Low-carb eating means not having enough energy since you don't have carbohydrates. Fact: Your body, even if you're very slender with zero perceptible fat on you, has enough fat in storage to run ten marathons without eating, yet you can't even run one with a maximum load of stored carbohydrate. Your stores of glycogen, which is what carbohydrate is metabolized into in the body, are limited to about 2,000 calories at most. Even the leanest person has five to ten pounds of fat stored on them (and most have a lot more) with each pound being 3,500 calories. You do the math.
- Myth: You need carbohydrates. Fact: There are no essential carbohydrates. There are essential fatty acids and protein complexes, along with ascorbate (vitamin C) that your body cannot synthesize, but no such thing exists for carbohydrates. The exact amount of carbohydrate your body requires is zero.
- Myth: You can't perform athletically without carbohydrates. Fact: Athletic performance, especially for endurance events such as running at double-digit mileages, is not only possible without carbohydrates it in many ways can be superior. During heavy exertion the digestive system is effectively shut down because the body shunts its energy resources to the skeletal muscles to drive that performance. Since carbohydrate stores are limited to about 2,000 calories and a mile of running requires somewhere between 100 - 120 calories to sustain plus your base energy requirement (another 150 calories/hour or so) during longer endurance events you're constantly "dancing with the devil" in attempting to consume carbohydrates and digest them while your digestive system is barely functional. If you lose this dance you either vomit or have an immediate need to relieve yourself out the other end -- and both of those events come with dehydration, which is very dangerous when exerting yourself heavily. By contrast when running on lipids (fats) even the leanest athlete has more than enough fat in their body to run several ultra marathons back-to-back and thus need consume nothing in the way of food, requiring only hydration and electrolytes that can be immediately absorbed by the intestines. Further, studies have shown that those who are low-carb adapted burn much more fat during exercise than those who run into glycogen-deficit due to lack of carbs during a workout. In other words if part of your fitness goals include losing or maintaining body mass then being keto-adapted, that is, eating low-carb, will make your exercise far more productive in terms of losing weight -- 2.3x as much, to be precise.
- Myth: There's nothing to eat, it gets boring fast, and nutrient quality is poor. Fact: See the below list; virtually everything available to eat before the introduction of cheap international transport and "factory" foods is compatible with low-carb eating. Any form of animal flesh, eggs, cheeses, most vegetables and modest amounts of fruit and nuts are what make up a low-carb dietary intake. In addition virtually all spices are zero-carbohydrate and can be used without concern as to quantity. When you eat a lot of carbohydrate you're targeting caloric intake since high-carbohydrate foods have very low nutrient levels. The poster child for this is of course sugar, which other than carbohydrate has essentially zero nutrients, but it doesn't end there. Most high-carb starchy foods have very low vitamin and other nutrient loads compared against foods such as broccoli, kale and similar. Broccoli, for example, has your entire Vitamin C and K requirements in one serving along with a very high nutrient and protein balance score yet nets only 31 calories per serving and 6 grams of carbs, 2 of which are indigestible (fiber.) Rice, on the other hand, has a very low nutrient balance score, a decent protein balance, 205 calories/serving (6.6x as much!) and 45g of carbs yet only one gram of fiber (1/4 as much.) It also fails to provide any material amount of your vitamin requirements; the only related item that measures reasonably-well is folate. On the other hand when you eat low-carb your nutrient levels are naturally very high since those non-animal-source foods compatible with low-carb eating are sparse in calories. In short, assuming you consume the same caloric intake, what you "crowd out" when eating high-carb is nutrition while what you "crowd out" when eating low-carb is junk.
- Myth: Low-carb means eating a very high amount of protein. Fact: Low-carb eating contains moderate protein levels. Very high amounts of protein in fact are not "low-carb" since protein, when taken in beyond metabolic needs, is converted to glucose in the body. That would be the opposite of what you're intending. Don't trim the fat off your steak, consume it instead.
- Myth: Your cholesterol balance will go to hell on a low-carb diet and you'll have a heart attack. Fact: HDL typically goes up and LDL typically goes down, which is good, not bad. However, there are several flies in the ointment of the common rubric regarding cholesterol, dietary fat and heart disease, not the least of which is that the correlation in several studies, including recent studies, has been backward. That is, increased carbohydrate and PUFA (polyunsaturated fatty acids -- read, vegetable oils) intake is associated with increased, not decreased, ischemic heart disease. Want to have a heart attack? Eat carbs and vegetable oils. Seriously, I'm not kidding.
- Myth: You won't stick with it even if you try it. Fact: If you really do keto-adapt it is unlikely you'll ever return to eating high-carb foods en-masse. Why? Because you'll find them to be too sweet and no longer tasty. Sugar and its analogues are quite-addictive, and like most addictive things their "dose response" goes down the more you use them. That is, after a while a given amount of sugar doesn't taste "sweet" any more, so you add more to get the same "sweetness." Stop consuming sugars for a few months and suddenly even a tiny amount tastes too sweet, and is no longer pleasant. In addition once you become keto-adapted you are no longer a slave to food. People are utterly shocked to find that I often wake up in the morning and have no desire to eat anything until somewhere around lunchtime! They wake up famished every morning and immediately hit the pancakes, cereals and breads. I did too, until I went keto-adapted and that all disappeared. If you've ever been "hangry" it's because you're actually experiencing withdrawal from the addictive nature of fast carbohydrates. If you enjoy being a slave then may the chains rest lightly on your back, but just remember that this form of slavery comes with greatly-increased risks of heart disease, obesity and diabetes. Are you sure it's worth it?
Once again, for those who missed it the last time, here's the "don't eat" list:
- Anything with added sugars on the label irrespective of amount. If a word ending in "-ose" is on the label, it's a sugar. Maltrose, dextrose, sucrose, fructose, etc. All are sugars. Go through your cupboard and throw all those packages and cans out, and don't buy any more of them.
- Anything with man-made PUFAs in it. There are two basic types of PUFAs -- Omega-3 and Omega-6. Omega-3 is good for you in reasonable amounts and is almost-exclusively found in the flesh of animals, including most-especially fish. Omega-6, on the other hand, is found naturally in most plant material. The problem is that the amount found in plants you eat whole is tiny but when concentrated into man-extracted oils from vegetable sources you wind up consuming thousands of times more of it than you ever could by eating the actual plant. Cottonseed oil, for example, is full of this stuff, yet you'd never sit down and eat a bowl of cotton seeds! Likewise, you'd have to eat something like two bushels of corn in a single sitting to get the amount of PUFA found in one tablespoon of corn oil, but it is utterly trivial to consume that amount in baked goods. This is true for all vegetable oils. The only exception? Small amounts of olive oil are reasonable used as a salad dressing. But you should never, ever, cook with vegetable oils including sauteeing, frying, basting or similar because the fact that they're unsaturated means they oxidize rapidly and heat makes them oxidize more and faster. The "switch" to vegetable-based oils in fryers has probably killed more Americans in the last 40 years than all other causes of death combined. By the way, if you want the worst of the worst they come in the form of anything that has the word "hydrogenated" on the label. Those are PUFAs that have been chemically stabilized so they are a solid and don't spoil while on the shelf in the store. Let me be crystal-clear: The amount of PUFA you can safely ingest, and thus should ingest, is zero, with the exception of room-temperature olive oil used as a salad dressing or similar. That section in your grocery store is IMHO "heart attack in a bottle."
- "White", starchy vegetables and plants. This means rice, potatoes and similar. Rice and potatoes are peasant food. If you'd otherwise die they're acceptable, I guess, but I'd hardly call them my first choice. Rice I've already covered but potatoes aren't far behind. Their nutrient balance is severely skewed and, frankly, sucks. With 63g of carbs and 278 calories in one large (300gm) potato, while they have a decent amount of fiber (7g) and a good protein balance the rest is lacking. Of the vitamin complex only C and B6 are well-represented, and only half of your needs (compare against Broccoli.) The real problem with starchy foods is that they're carb-dense but nutrient-poor on balance which means they're not only incompatible with low-carb eating they will probably crowd out the nutrient-dense vegetables you should eat. Since these tend to digest quickly they also provoke a large insulin response. Note that any of these fried in PUFAs, such as french fries, dramatically multiply the trouble. These "foods" are served in restaurants (e.g. xxx "over rice" or xxx "with fries") because on a per-calorie basis they cost almost nothing.
- Grains (especially wheat) and anything made with them. Cereals and similar are even worse than starchy vegetables in that the fiber is nearly-all absent as processed and thus has to be added back. Whole-wheat bread has a horrible protein quality score, is very high in carbs with 2 slices having 24g all on its own (20 of which "count" as there are 4 of fiber) and a modest nutrient balance. Store-bought breads and cereals, however, almost all contain hydrogenated oils -- that is, the worst sort of PUFAs. In terms of insulin response grains are almost-indistinguishable from table sugar and some are actually worse. Yes, this means no pizzas, pastas and similar. Again, the reason that hamburger comes on a bun at the restaurant or drive-thru is because on a per-calorie basis it costs pennies; to get the same calories with that burger wrapped in lettuce you'd need another patty that contains actual food.
So what do you eat?
- Green vegetables such as spinach, kale, broccoli, brussels sprouts, cucumbers, etc. All are high in nutrients, low in calories, very low in carbohydrate and glycemic load and most have a good amount of fiber as well, all of it being naturally-occurring (not "added back.") Frozen is fine; fresh is ok if you prefer it but there's no nutritional difference that's material. Update: Oxalates are potential trouble for some people even in small amounts, and in very large quantities probably trouble for many. Spinach is one of the few green vegetables with high levels of that specific compound so you might want to avoid it.
- Modest amounts of fruits are fine, eaten whole, approximating what you could obtain in season. Note that neither fruits or vegetables should be "juiced" or otherwise processed; doing so grossly speeds up the absorption of the sugars and destroys much of the fiber value! Eat your strawberries, in other words, as strawberries, not as a component in a "smoothie."
- Full-fat cheeses are perfectly ok; they have a near-perfect (75-80/20-25) balance of fat:protein. Do not buy the "reduced fat", "2%" or similar cheeses.
- Eggs likewise have a decent balance of proteins and fats, eaten whole, although they are a bit protein-heavy. Eschew the "eggwhite" and "eggbeaters" nonsense; break actual eggs and prepare them as you wish (it's perfectly ok to cook them first if you want them hard-boiled!) On mass eggs have about 6 grams of both fat and protein, but since fat is 9 cal/gm the energy balance (which is what you care about) is 1.5:1 in favor of fat. This means about 40% protein, 60% fat when you do the math; the goal for a non-athlete is around 20-25% of intake from protein, so they can't be your primary source but they're good overall.
- Full-fat meats and fish. Pork, chicken, beef and similar are all fine but do not trim or remove the fat portions. This means you eat your chicken skin-on, eschew the "skinless" chicken breast in favor of the complete version and eat it all. For steak, consume the fat and do not trim it; same with pork. For fish prefer fatty fish such as salmon and tuna.
- Reserve your excess fat, especially from bacon and sausage cooked for breakfast, and use it for cooking purposes -- such as sauteing or even microwaving vegetables. If poured into a coffee mug it will keep for several months in the refrigerator without a problem. If you're older than 40 your mother probably did this and she knew what she was doing. For other cooking purposes (e.g. if you want to have an omelet and don't happen to have handy reserved bacon fat) use butter. Coconut oil, incidentally, if you can find it without extra crap in it, is mostly saturated fat and is one of the very few exceptions to the "no vegetable oil" rule that can be used reasonably-liberally. Be careful buying it however as much of it is stuffed full of hydrogenated crap which turns it into one of the worst instead of being in the "acceptable" column. READ THE LABEL.
- Use all the spices you wish. Virtually all of them are zero-carb and zero-calorie. The same is true for hot sauces and such, but check the labels to make sure they're not stuffed full of sugars or hydrogenated oils. Most are not but there are exceptions.
If you eat this way it is very hard to exceed 50g/carb a day. As an example a cup of brussels sprouts has eight grams of carbs, only five of which count (3 are fiber and don't digest.) If you eat a cup of those, two cups of broccoli flowers during the day in various snacks (8g more), one cup of green sweet pepper chopped up as a component of a main course or side for dinner (4g net) you'll have eaten quite a decent amount of vegetables yet you only consumed 17g of carbs net all day; you'd also have consumed just 108 calories. You could triple that and still be ok on the carbs and yet have consumed just about 1/6th of your caloric intake requirement!
It then becomes a matter of choosing protein sources without trying to limit fats and, in fact, buying the cheaper sources tends to work better because the stores charge more to trim or otherwise remove the fats! Between eggs, cheeses and animal products while intentionally leaving the fat content present you'll wind up with a low-carb diet that is very rich in nutrients and almost-completely absent in insulin-spiking carbs that also happens to be free of PUFAs that are associated with heart disease.
Oh, and you won't be hungry either; your body knows how to regulate its food intake all on its own if you simply stop poisoning the signalling pathways (largely mediated by leptin) that tell you whether you're hungry or not.
Welcome to waking up and not really wanting anything to eat until the middle of the day; a nice side effect of living this way is that your pants will fall off.
The so-called "authorities" on health all admit that half of all adults are metabolically compromised (in terms of insulin resistance) with most of those over 65 being in this situation.
Being metabolically compromised places you at a materially higher risk of diabetes and heart disease. These are diseases that may kill you, but even if they don't they are debilitating. Obesity is a big part of that; you can't run, you can't move, you wind up with joint replacement surgery as you age (which has to be re-done every 10 or 20 years and is major surgery) and, if it gets out of control it can and will lead to amputations, blindness and ultimately kidney disease and dialysis.
This is a miserable way to live the last 20, 30 or 40 years of your life and it's not a pleasant way to die either.
Most people will say "well, I have no symptoms and my doctor is ok with what I'm doing", so they'll ignore the possibilities here. This is extraordinarily unwise as the damage that causes these diseases happens over years or even decades before clinical disease (that sends you to the doctor) presents itself.
It is easy and inexpensive, however, to know if that damage has accrued to the point that some detectable signs are present. You can do it at home, and you should because once these markers get into your medical chart they never go away and while people may think they're protected by Obamacare right now until and unless we deal with the medical monopoly situation in this nation you are risking financial ruin without cause if those markers get into your chart even if you reverse the damage.
What happened before Obamacare and will happen if and when it collapses? If those markers are in your chart you may become completely uninsurable at any rational cost. That means that any major medical emergency instantly bankrupts nearly anyone.
As an aside I'm going to make an assumption here: You're not diabetic today (diagnosed.) If you are diabetic then none of the below is news to you in terms of testing as you already have these results over time since they're part of what your doctor has you doing already. Nonetheless, you might be shocked at the improvement from the below eating pattern changes, so keep reading -- just ignore the testing thing, as you're already doing it.
This is something you can do in the privacy of your own home with nobody but you having the results. You can then change your behavior, specifically, what you do and do not eat, if you have a deteriorating situation and see if it improves. There is little cost to this, essentially zero risk over the time involved and if it doesn't work for you or if you think I'm a crackpot (I don't have an "MD" after my name, after all) you will have lost nothing other than a few dollars that were spent on something you probably ought to own anyway, one of which is not consumed.
You're going to go buy two things:
1. An A1c test kit. WalMart has them and they're under $30. There are two tests in the box, so each is about $15. No, one isn't for your SO, spouse or kid -- they're both for you. If you have two people to check buy two. These are consumed and tossed when used up.
2. An inexpensive glucose meter and a box of lancets. Buy one of the models with inexpensive strips; the meters are all cheap (~$20 or so) but the strip cost varies widely, by as much as 500%! While you're not using this for diabetes monitoring this is a device that will last years if not a decade or more so strip cost does matter, although not nearly as much. Again, WalMart has a wide selection -- IMHO make yours based on the strip cost (lower is better) and choose one that has individually-wrapped strips (this way they do not deteriorate by having a bulk package opened, since you are not using these multiple times a day as a diabetic would.)
When you get home open up the A1c kit, read the instructions (yes, you have to follow them to the letter to get good results) and run one. Keep the second. Write down the result.
The ADA and "some" docs say any A1c number under 6.0 is ok. You want a number at or under 5.6%. Note that these kits as with all tests, including lab tests, have an error band to them which means that one test provides decent information but you need to check it as the actual number could be a few tenths to either side of the displayed result. Don't use the second test immediately (unless the first errors out due to a mistake on your part); you'll use that a month or two down the road to both check the error band (the odds of a random error going the same way twice is 1 in 4 instead of 1 in 2) and your outcome.
Be aware that there are some confounding factors with the A1c test. First, it "assumes" blood cells live three months. We know this is not always true; people with severe metabolic damage tend to have them live for less (which means the number reads low) and those without said damage tend to have them live longer (which means the number reads high) since what A1c measures is the percentage of glycated hemoglobin in the blood. Further, if you have some conditions, among them anemia (in particular) it will read low because in that case hemoglobin is below normal levels -- this is a particular risk for women who don't get enough iron in their diet although there are other causes. This probably won't change your test result enough to matter, but it is the reason that standing alone an A1c test, while good and in fact an essential checkpoint, isn't enough.
Next, you're going to do two different checks with the glucose meter. The first is a fasting test, which is done when you first wake up in the morning before eating or drinking anything other than water. Most meters will store some amount of history but again, write it down. If your number is under 90 but greater than 50 that's ok. If it's under 50 test it again -- a persistent result under 50 is an indication of hypoglycemia (low sugar) which is dangerous as levels below 40 can cause you to pass out (and if nobody finds you and deals with it you can die), so if you get a confirmed reading under 50 consider obtaining medical advice. Again, the ADA and some docs say anything under 100 is ok. Correct clinically but wrong for the purpose you're intending here. If you get a number over 90 do it again the next day; if you get a second reading over 90 you've got a potential problem.
The final thing you're going to do is wait until you eat a "normal" meal at home (whatever that is) but it should include a decent amount of carbohydrate. "Decent" doesn't mean carb overload, but it does mean roughly the equivalent of one cup (cooked) of rice. If you eat low-carb normally, this is your chance to eat something you usually don't. Test your blood sugar level before eating, then test again both one and two hours after eating. Write down the results; no relying on memory here. You should not get a result over 140 on either of the post-eating tests and ideally within two hours you should be back to where you were before consuming the meal. If you're not, take a third test at the three-hour point.
Now let's interpret.
If you are eating food containing carbs on a regular basis, your A1c is at or under 5.6 and your fasting glucose is under 90, neither of the one and two-hour post-meal readings exceed 140 and you are back to baseline within three hours you are probably ok metabolically at this point. This doesn't mean you don't have insulin resistance of some amount but at this point it is not manifesting in clinically-detectable harm to your cardiovascular system. If you are eating low-carb and have been for several months or longer your fasting glucose level may be a few points higher, anything under 100, and is ok provided the other two tests are both in-range. Note that if you are overweight you probably are metabolically compromised (an OGTT w/insulin assay would easily detect it) but the test is expensive and frankly, the mirror works just as well for anyone in this category: If you have a gut, you're metabolically compromised. Incidentally just because you eat low-carb you are not necessarily going to get a somewhat-higher fasting glucose level; I don't, for example, and I've been eating low-carb now for something like five years now but some people do. If you are eating low-carb and get a reading over 90 for your fasting glucose there is a decent chance you're doing it wrong; specifically, you may be eating far too few green vegetables in an attempt to go "very low or zero carb" and thus massively short on vitamin and mineral nutrients. It is possible to eat "VLC" and not have this problem but severe nutrient deficiencies play hell with hormone levels, so don't just blindly accept that an elevated fasting level is "ok" -- it's not, and it usually means you're doing something wrong and accumulating damage.
If your A1c is over 5.6 (but under 6.0) or your fasting glucose is over 90 (over 100 for low-carb eaters) or your first two-hour post-meal readings (either or both of them) go over 140 or you are not back to baseline within 3 hours you are accumulating metabolic damage that is doing material harm to your body. Your doctor will probably not detect this in his routine screen but if you ran the (expensive) OGTT w/insulin assay test, which your insurance will not cover in this instance since there is no clinical indication of disease, I'll lay a large wager it would show significant metabolic compromise with insulin levels perhaps as much as twice normal levels. You're at severe risk down the road even if you are not overweight and if you are overweight you're a walking heart attack or stroke unless you change what you're doing. More than half of all adults in the US and most people over 65 are in this category or one of the worse ones below.
If your A1c is over 6% or fasting glucose is over 100 (irrespective of what you eat) or either of the first two post-meal readings is over 160 (you almost-certainly won't be back to baseline within 3 hours in this instance) you're either diabetic now or shortly will be. Your doctor will be able to detect this in a routine screen; if he's honest he'll call it "pre-diabetes" and if he does your medical chart will be "branded" forever which, to the extent legal now or ever again, will trash your ability to obtain health insurance at a rational cost. You'll also get a whole raft of pills shoved at you, probably including metformin (to start) and a statin. That's the traditional thing for them to do but it may be both harmful and unnecessary.
If your A1c is over 6.5% or fasting glucose is over 130 or any of your post-meal readings are over 200 you are in trouble as you are almost-certainly clinically diabetic now. This pretty-much meets the "bright line" test in the medical establishment to call you diabetic. If this is the case your chart and impact on health insurance is irrelevant if you change nothing as it is a virtual certainty you will if not are suffering real, material and serious damage to your health. You're probably symptomatic too but denying it. It is your call what to do with that information but before you run to the doctor for a formal diagnosis and permanent branding on your medical chart, assuming you haven't previously been diagnosed, read the rest of this article.
If you're of both of normal weight and your results are in the first category then relax -- and in a year, or if you become overweight, do it again just to keep tabs on things.
But let's assume you are either (1) overweight or (2) your results are in any of the bottom three categories irrespective of your weight.
Try the following for a short period of time (4 weeks):
1. Stop eating sugars of any sort. If it says "sugar", "fructose", "sucrose", "corn syrup", "hfcs" or anything of the sort anywhere on the label do not eat it. No more cookies, no more chocolate, no more sugar in the coffee, no sugared sodas, etc. Just stop. No exceptions, no tapering down, stop.
2. Stop eating starches and grains. No more pastas or potatoes of any sort. No more bread irrespective of the type.
3. Stop eating anything containing machine-processed vegetable oils. No more corn oil, canola, rapeseed, etc. No cooking with any of these oils and yes, that includes peanut oil; the only exception is olive oil as a salad dressing (e.g. with vinegar.) This crap is in a lot of "food" and no amount of it is healthy. This means no more packaged foods in the general sense; no more boxed dinners, canned ravioli, "lunch pouches or easy-prepare things" and similar (those probably break all three constraints!), nothing that comes in a bag (other than frozen vegetables), etc. This also means no fried food of any sort prepared away from home since essentially nowhere fries anything in either tallow or lard any more (but they should.) If you like wings find a place that bakes them and order them with the dry rub instead of the HFCS-laden sauce.
These three rules above are absolutes. You'll be tempted to cheat, but we're talking about a month here. Just don't; you can do it, and you know it.
Now on to what you do eat.
4. Do eat all the green vegetables, whole, not canned or packaged, you want. Find something or a bunch of somethings you like such as broccoli, brussels sprouts, bell peppers, lettuce and similar. Whole, fresh or frozen (e.g. in a bag) are fine; canned or otherwise processed are not. Substitute these any time you would otherwise eat any sort of snack and keep eating them until you're not hungry any more. It's not impossible and it won't hurt you; in fact, they're all good for you. It is close to impossible to overeat if you're consuming green vegetables.
5. Do eat full-fat protein. Pork, chicken (skin-on, not trimmed), steak, hamburger (no bun; that's grains), fish, eggs, cheese, etc. No restrictions on any of these foods, but eat when hungry until you're not, not until "full."
6. Use spices, including pepper, cumin, etc. as much as you wish. Hot sauces typically contain zero sugar and are perfectly fine even in wild amounts (yes, Tobasco is ok.) This is a taste-based thing, of course, but anyone who thinks you can't toss on the Lowrey's or pepper the hell out of your steak is flat-out wrong. Not only can you use salt unless you are one of a very small percentage of the population that has a genetic intolerance to sodium restricting salt intake is worse than worthless in that electrolyte imbalances lead to cramps (especially if you exercise) and can be dangerous.
7. Be careful with legumes and nuts. These are generally ok but nuts are very high in caloric content and it's easy to wind up eating 3,000 calories worth of them in a few minutes! So if you want a few as a snack, go ahead; just don't eat them as a meal rather than as a snack. But do not generalize this to nut-based oils (such as peanut oil) or anything processed from nuts because you are then concentrating the bad without the balance of the good (see above in point #3.)
8. If you normally consume alcoholic beverages keep it to one per day on average and not more than two on any day.
9. Drink any time you're thirsty; water is of course ok, if you like coffee go right ahead. Cream is ok (not non-dairy creamer, actual cream that has to be in the fridge) but sugar is not. If you want sweetener use any of the non-sugar ones (we're not going to be a nazi about these for this purpose.) Diet sodas may be ok, but if you can avoid them do so.
Do this for one full month.
Now repeat the above tests. Note that A1c typically measures average blood glucose levels over about a three month time frame, so the change there may not be dramatic and in addition the error rate on the test may obscure the results.
But remember the above table; if you drop a category or approach doing so you have hard proof that you required no medication whatsoever to improve your situation and these results are individual to you.
In other words you didn't read something on The Internet by some kook (like me), you didn't take blind advice from some doctor or nutritionist (irrespective of how many letters are after his name) you ran an individualized test with objective results on your particular genetic and metabolic make-up and have a set of numbers before you that document the outcome in your particular body.
If the results show no change (or get worse) then you've lost nothing other than a bit of time and a few dollars. Over this short of a period of time no harm is going to come to you; the harm that comes from bad metabolic markers in this regard requires years of accumulation before it "gets" you. But if the results are either dramatic or trend the right direction (and if you actually do the above it's a good bet they will) you now know that it is possible to change those objective metabolic markers through near zero-cost measures that are easily implemented in your daily life without spending one minute in a doctor's office or taking (and spending money on) one single pill.
Is that enough motivation to continue for another month or two and see if you can return your metabolic profile to the top, that is, "ok" category?
Further, you just prevented yourself from being "branded" in your medical chart and you didn't do it by cheating, you improved your actual metabolic profile.
That ought to be plenty of reason to continue on that path and make it a lifestyle, considering that the difference between said improvement to the top category and any of the others is a very material change in your risk of heart attack, stroke, blindness, amputation, dialysis and death! Further there's a very good chance that at the same time you're going to see a change on the scale if you're overweight, and I bet you'll like that change as well.
If this proves up it is going to be an absolute disaster for everyone in the health field -- in fact, it will be as bad as the disaster that resulted from exposure of the fact that leeches were worthless in "treating disease."
Coronary Artery Disease, or "CAD" for short, has proceeded from the following general premises:
1. Cholesterol in the blood binds to sites of inflammation in the artery, treating it much like it would a splinter in your foot.
2. That process is cumulative and, over time, blocks more and more of the artery.
3. Eventually this produces a blockage that either breaks off (a stroke) or you have a heart attack due to insufficient blood delivery to the heart muscle.
In fact if you look around Google for "Coronary Artery Blockage image" you will find hundreds of images that look like this:
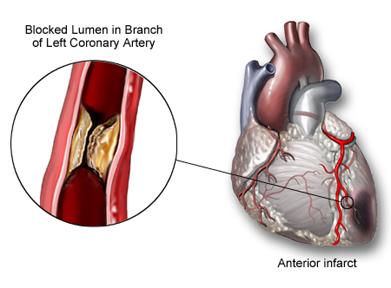
There's one problem -- they're all wrong.
The paper cited above points out the logical fallacies that have attached to the "common model" you're taught and that your doctor -- and cardiologist -- is using.
- This is a systemic disease, that is systemic inflammation is usually believed to be the root cause and it makes sense, except for one problem that this paper points out: The only place the arterial blockage tends to occur is in the cardiac arteries; the entire rest of the body appears to be either entirely unaffected or almost-entirely so. It is exceedingly improbable that systemic inflammation would leave all the other arteries in the body untouched yet selectively clog the ones around the heart. Indeed, every cardiologist knows this; where do you think they get arterial grafts from (usually veins in the leg) and how many of those do you think the average cardiologist has seen, and how many have asked "how come this one's not blocked too, given that it's a similar-sized blood vessel?"
- If high LDL-C levels produced CAD then removing the high LDL-C levels by any means (including drugs) would eliminate the disease. It does not; only about 30-40% of those at risk are "helped" and plenty of people with "normal" LDL-C levels get CAD. This means that the presence of LDL-C cannot be the cause of CAD since eliminating the presence of the alleged causative factor does not eliminate the disease.
- Invariably, as in the above image, the plaques are shown initiating at the arterial wall and growing inward. The problem is that this isn't what actually happens; the first depositions of LDL-C take place deep inside the arterial wall and there are few molecules present at the blood/wall boundary. This I was not aware of and you probably weren't either, given the above image that everyone has in their head that's ever looked at one along with the accompanying text. Guess what: That image and text is factually incorrect.
Now let's add some more facts to the mix that are discussed in the paper:
- The coronary arteries develop a multi-layer structure early in life through cellular differentiation that thickens until young adulthood, then stabilizes, maintaining itself thereafter. That is, this normal state develops in all humans over roughly the same time frame (immediate post-birth through age 30 or so.) Contrary to the common presentation the inner layer is not a single layer of cells; it is a multi-layer structure.
- There is a substance, proteogycan biglycan, that binds to LDL-C and is normally present in the outer layers of the coronary arterial wall. By contrast the inside layers are poor in this substance. However, the outer layers of the inside arterial wall cannot access LDL-C from the bloodstream flowing in the artery because the arterial wall is normally not vascularized -- that is, there are no capillaries bringing blood to it. Instead, oxygen and glucose reach these cells via direct diffusion. LDL-C is too large to diffuse through that distance in any material quantity irrespective of its presence in the blood.
- LDL-C does not accumulate starting at the inside arterial wall outwards. This effectively demolishes the claim that it is via the blood flowing in the artery and diffusion that such deposits are picked up and accumulate; it is logically inconsistent since to reach those outer layers the inner ones must be reached first!
- It is known that one of the reactions to oxygen starvation of cells is to stimulate vascularization. That is, when cell layers get too thick for diffusion to work any more they stimulate the development of capillaries to bring them oxygen and transport both glucose and waste.
- The appearance of vascularization always precedes the development of CAD and originates not from inside the inner arterial wall but rather from the outside in; in arteries where it is not present no plaque development occurs.
- This abnormal vascularization and concentration of LDL-C are observed in other tissues. Specifically, this has been observed in the cornea which is also normally not vascularized but, if it becomes so, fatty plaque formation occurs. This has been known for 50 years and yet has been ignored in the CAD "debate."
- Arterial plaques in the coronary arteries are more common in herbivores than carnivores, and occur in all eutherian (placenta-bearing) animals with a body mass comparable to or larger than humans. You've been told that CAD is a uniquely-human disease and meat-eating is more-dangerous in this regard than veganism. The claim that CAD is a human disease is a bald and knowing lie, and further herbivores are more susceptible to the disease than carnivorous eaters! So much for vegetarianism being protective against heart disease.
This paper roundly demolishes a number of claims that are made every day in the media and the medical establishment, and what's worse is that it completely decimates the balance of benefit and harm argument for the use of drugs to "lower cholesterol" such as statins because once the inner coronary arterial wall has become vascularized LDL-C will inevitably be picked up and accumulated.
Let's put forth what is directly attacked and, if this paper holds up, refuted:
- Coronary Artery Disease is a human condition. False; it is found in all placenta-bearing mammals of human or larger size.
- Coronary Artery Disease is a condition that is more-common and more-severe (or even exclusively present) in meat-eating animals. False; it is in fact more-common in herbivores than carnivores. That is, there is zero evidence that vegetarian eating is helpful and in fact the evidence among animals in general goes the other way.
- Coronary Artery Disease is caused by LDL-C. False; greatly attenuating LDL-C does not prevent the disease; it is at best 30-40% effective.
- Coronary Artery Disease begins with LDL-C carried in the arterial blood that diffuses through the inner arterial endothelium directly. Not likely; that is not a single-cell layer as commonly depicted, and the concentration of LDL-C is higher in the deeper layers, which is logically inconsistent with that claim. Further, CAD does not present in arteries that have not had the deeper layers vascularized which is logically inconsistent with the theory that LDL-C in the arterial blood deposits on or diffuses through the arterial wall.
The problem with what's presented here, from a medical perspective, is that if this paper proves up it doesn't leave you with a trillion dollar industry you can force people to spend money on by scaring them to death.
If in fact the growth of the inside layer of your coronary arteries in thickness is a risk factor that simply comes with time on the planet then given the inherent response of cells that become less-than-well supplied by oxygen (that is, to stimulate vascularization) there may be no actual cure available for this condition; it may simply be inherent in getting older, with some people more susceptible than others.
If, on the other hand, there is some sort of systemic insult responsible for the thickening of these inside walls beyond the limits of diffusion to provide transport that might be able to be addressed. The problem with such a belief is that you then have to find the same insult pathway -- whether from the same cause or not -- in the other mammals that also suffer from the condition. That becomes a rather serious problem since obviously other large placental mammals don't eat trans-fats or refined sugars, as just one example.
In short while this paper is a not a smoking gun as to cause it refutes a lot of false claims about coronary arterial disease and, if it holds up to scrutiny you may be witnessing the imminent destruction of a trillion-dollar a year scam.
Stay tuned.
PS: This paper's description is also consistent with why smoking promotes (but does not cause) coronary artery disease. Smoking raises CoHb levels, which in turn would tend to lead to cellular hypoxia, with the most-severe effects being in cells where the diffusion path is the longest. That, in turn, would be expected to promote vascularization..... Likewise, it explains the association between sleep apnea where depression of oxygen saturation has been documented and CAD -- an association that has been shown but I've yet to see a plausible scientific explanation as to why they're associated. This definitely appears to merit further study!
If you "diet" you will fail. You will fail because you never changed anything in the long term, and as soon as you go back to what you were doing the same result will come. What else can you reasonably expect?
If you have been reading the newspaper recently, you will have come across some startling new nutrition advice. A much hyped new study, conducted with just 150 participants, calls for us to “embrace fat”—even the saturated kind. The alleged benefits? Weight loss and, most incredibly, healthier hearts.
No kidding? Well, he thinks it is kidding.
In the two centuries during which these diets have been promoted, there have been hundreds of studies comparing low-carb to low-fat diets. One would think that by now it would be clear which was superior if there really was a difference. But if you take all of these diet studies, and analyze the enormous body of data they produced, there is no proven difference between them as far as weight loss is concerned. In fact, another such analysis was published the day after the over-hyped low-carb study with this same conclusion.
If you're looking for a diet, that is, something faddish you can do that will produce result "X", you can find it whether it's straight starvation or something else. Then there's this:
More to the point, however, is that this most recent study really did not actually prove that low-carb diets are superior. The low-fat diet in the study was not that low in fat, and the low-carb group ate significantly fewer calories.
Well duh.
See, people keep missing this -- it's a lifestyle choice, not a diet.
Do you eat fewer calories? Yes. You want to know why? Because you're not hungry, that's why.
There's no magic to it. When you're hungry if there is food available you'll eat, all things being equal. Oh sure, you can apply extreme willpower to counteract that, but will you succeed? Probably not at all, and almost-certainly not for long.
So what's the secret? It's easy -- don't be hungry.
That's what low-carb does, you see.
Sugars and things that quickly convert to sugar produce a "high." Ask any parent about their kid being jacked up on sugary things. Well if you've all seen this why do you think it doesn't happen to you?
And what comes after that when you "come down"? The crash, of course, and what do you want? More of what made you high.
Is it really any more difficult to understand than that?
Nope.